A wound healing assay is used to evaluate cell migration by measuring how cells move to close an artificially created gap over time. It is commonly applied to study wound repair, tissue regeneration, and mechanisms related to cancer metastasis.
Celloger® Pro performs automated bright-field time-lapse imaging directly inside the incubator, capturing images every 30 minutes for up to 72 hours. This enables continuous, real-time monitoring of wound closure without disturbing cell culture conditions.
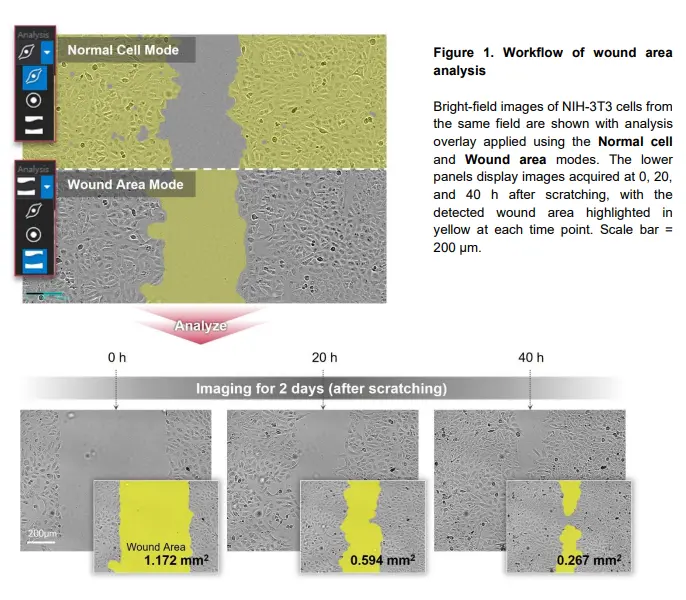
Wound closure is quantified by measuring the wound area at each time point and calculating the percentage reduction relative to the initial wound area. The Celloger Analysis App uses an image-based algorithm to automatically segment the wound region and compute closure rates.
In this application note, wound healing assays were monitored for 72 hours with images acquired every 30 minutes. This duration allows both early and late-stage wound closure dynamics to be captured.
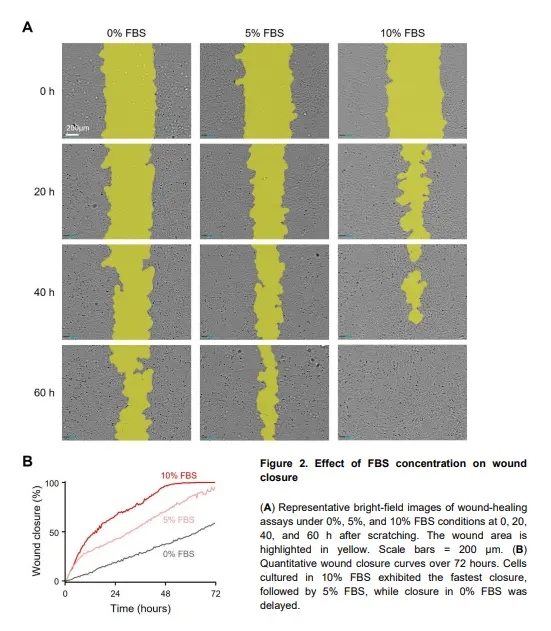
Higher FBS concentrations accelerate wound closure by enhancing cell migration and proliferation. Cells cultured in 10% FBS showed the fastest closure, while 0% FBS resulted in delayed and minimal wound recovery.
NIH-3T3 mouse fibroblasts were used in this study. These cells are widely used in migration and wound healing assays due to their robust and reproducible motility behavior.
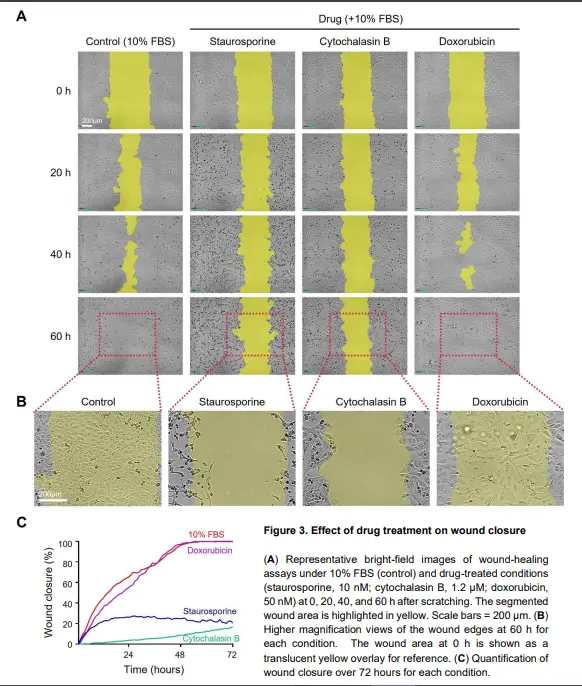
Migration-modulating drugs produced distinct wound closure patterns depending on their biological effects. Staurosporine halted closure due to apoptosis, cytochalasin B reduced closure by disrupting actin dynamics, and doxorubicin maintained closure despite suppressed proliferation.
Celloger® Pro automates image acquisition and wound area analysis, reducing user-dependent variability and improving reproducibility. It also enables standardized, long-term time-lapse imaging across multiple experimental conditions.
Yes, the advanced wound detection algorithm provides accurate and consistent segmentation even in low-contrast or partially closed wound regions. This improves the reliability of quantitative analysis throughout the assay.
These assays are useful for regenerative medicine, cancer research, and cell motility studies. Celloger enables clear comparison of migration responses to serum conditions and drug treatments with minimal manual intervention.
Download the full Application Note PDF
to gain comprehensive insight into the automated wound healing assay workflow, including real-time Celloger® Pro imaging, quantitative wound closure kinetics, and comparative analysis of cell migration under varying serum conditions and migration-modulating compounds in NIH-3T3 fibroblasts.